Women develop diseases differently; they exhibit different symptoms, have different risk profiles, and go through life stages—such as pregnancy and menopause—that place particular strain on the cardiovascular system. Yet many guidelines, studies, and diagnostic thresholds are still based on data from male patients.
The consequences are serious: cardiovascular diseases are diagnosed later in women, are less often correctly classified, and are more frequently treated in a manner that does not adhere to guidelines.
At the German Heart Center at Charité (DHZC), we are therefore establishing gender-specific cardiology. We combine clinical experience, interdisciplinary care, and cutting-edge research to consistently account for gender differences—from prevention through diagnosis to treatment.
Because good cardiology is not gender-neutral. It takes differences into account—for individualized, personalized, and holistic care.
Women and men differ in various ways, including genetically and hormonally. These differences also affect the cardiovascular system:
- On average, women have smaller hearts, lower stroke volumes, and narrower coronary arteries.
- The heart and blood vessels respond differently to stress and aging.
- The female hormone estrogen has a long-lasting protective effect on the heart: It promotes vascular health, has anti-inflammatory effects, and influences metabolism, blood clotting, and blood pressure regulation.
As a result, cardiovascular diseases occur on average ten years later in women than in men. Women often have more comorbidities at the time of diagnosis, which can complicate diagnosis and treatment.
Living conditions, social roles, and access to medical care also play an important role:
Women and men describe symptoms differently and, in some cases, have different priorities and obligations in their daily lives. Women perceive preventive care services differently and are often examined later or less thoroughly by medical professionals.
Although women utilize preventive care services more than men, they often forego more extensive medical treatments and check-ups—in part because they do not want to be absent from work or personal life any longer.
The result: cardiovascular diseases are more frequently overlooked or detected too late in women.
- Autoimmune diseases occur significantly more frequently in women—which also increases the risk of cardiovascular disease.
- Medications work differently in women: At the same dosage, they often have higher levels of the active ingredient in their blood.
The result: Side effects occur up to 70 percent more frequently in women than in men, and dosages often need to be adjusted.
The Reality of Care Today
Although knowledge about gender-specific differences in cardiology is growing, women remain underrepresented in clinical trials.
The result: Many treatment recommendations are based primarily on data from men, and care is provided according to a “one-size-fits-all” approach. Women-specific factors are still not given enough consideration.
What needs to change
- More research specifically on women’s health and gender-specific cardiology
- Better consideration of gender-specific differences in guidelines and studies
- More knowledge about women’s cardiology in education and practice
Our goal: More personalized, equitable, and better care for women and men with cardiovascular diseases.
“Women are not simply ‘female men’: they develop illnesses differently, exhibit different symptoms, have different risk profiles, and go through life stages—such as pregnancy and menopause—that can have a particular impact on the cardiovascular system.”
Dr. Julia Lueg

“Women are not simply ‘female men’: they develop illnesses differently, exhibit different symptoms, have different risk profiles, and go through life stages—such as pregnancy and menopause—that can have a particular impact on the cardiovascular system.”
Dr. Julia Lueg
What is gender-specific cardiology?
Cardiovascular diseases manifest differently in women and men, progress differently, and sometimes require different treatments. The goal of gender-specific cardiology is to specifically incorporate these differences into diagnosis, treatment, and prevention.
Risk factors also differ between the sexes: hormonal influences—especially before and after menopause—play an important role. In addition, certain risk factors such as diabetes or high blood pressure often have a greater impact on heart health in women.
A major reason for existing knowledge gaps is that women have long been underrepresented in medical studies. Under the Food and Drug Administration (FDA) in the U.S., women were completely excluded from participating in Phase I clinical trials between 1977 and 1993 (Moley 2024).
In Europe, this has only been the case since 2001 and in Germany only since 2004 that an appropriate representation of (biological) genders in clinical research has been demanded.
Hormonal fluctuations or pregnancy as vulnerable and sensitive periods in a woman’s life make it difficult to include them in studies. Women continue to shoulder the bulk of family “care work,” which also reduces the resources available for study participation on the part of the patients (Sources: Vervoort et al. 2024; Berro Rivera 2025; Frew et al. 2014).
The result: Much of the knowledge regarding heart disease, diagnostics, and treatments is based primarily on data from men—and is not always directly applicable to women. But women are not just men with female bodies.
Gender-specific cardiology helps to better understand these differences and take them into account in medical care. This is intended to improve the detection of heart disease and enable individually tailored treatments.
Our goal: More precise, personalized cardiology – for better care for women and men.
“Our goal is to identify risks early on, prevent complications, and protect patients’ heart health in the long term.”
PD Dr. Kun Zhang
“Our goal is to identify risks early on, prevent complications, and protect patients’ heart health in the long term.”
PD Dr. Kun Zhang
Risk factors and situations associated with cardiovascular disease
Gender-specific differences play a particularly important role in assessing the risk of cardiovascular disease. The classic risk factors can have varying degrees of impact depending on gender. In addition, there are risk factors in women that do not affect men—for example, because they occur during pregnancy.
Family history also plays a major role. For example, women under 65 have an approximately fourfold increased risk of a heart attack if their mother has coronary heart disease—significantly higher than men of the same age and in a similar situation. (Haider et al. 2020).
These specific factors should be taken into account when assessing personal risk and in preventive care, especially for women.
Classic risk factors
At a young age, women are less likely to be affected by high blood pressure, but as they get older, the ratio reverses. 70 to 80 percent of women over the age of 60 have high blood pressure, and their blood pressure often rises more rapidly.
After menopause, high blood pressure is even the most common cause of cardiovascular disease and death among women.
The risk of coronary heart disease is similarly high in both women and men due to high blood pressure. In younger women (ages 40–50), however, elevated systolic blood pressure in particular can increase the risk of a heart attack. In addition, women’s hearts react more strongly to elevated pressure: the heart muscle thickens more frequently, and the heart’s ability to relax can deteriorate.
In terms of treatment, there are few differences in the effectiveness of medications. However, women are more frequently prescribed diuretics, while men are more likely to be prescribed other blood pressure-lowering medications such as ACE inhibitors or AT1 blockers.
Important: Women experience side effects more frequently, such as a dry cough from taking ACE inhibitors or fluid retention with certain medications. Treatment often needs to start with lower doses for women so that they tolerate the therapy well and can continue taking the medications.
High blood pressure can also occur during pregnancy—in about 5 to 10 percent of all pregnancies worldwide.
A serious condition during pregnancy is preeclampsia. Affected patients suffer from high blood pressure; often, other organs such as the kidneys, liver, or brain are also affected. Preeclampsia is one of the leading causes of preterm birth and complications surrounding childbirth.
Before menopause, women generally have a more favorable cholesterol profile than men:
- “bad” LDL cholesterol is lower,
- “good” HDL cholesterol is higher.
After menopause, LDL cholesterol in particular rises significantly in women. Low HDL and high triglycerides are particularly important risk factors for heart disease in women.
The good news: Cholesterol-lowering therapies (e.g., through the use of statins) work just as well in women as in men, both for prevention and after existing cardiovascular diseases have already developed. They can significantly reduce the risk of heart attacks and other cardiovascular events. The same target values currently apply to women as to men.
Important to know:
- Women experience side effects slightly more frequently, particularly muscle pain, when taking statins.
- In such cases, switching medications or adjusting the dosage may help. With statins, the nocebo effect also plays a major role: It refers to negative health effects that arise solely from the expectation of negative consequences, without a direct causal link to statin use.
- Other medications such as ezetimibe or PCSK9 inhibitors show no relevant differences between the sexes.
Despite the proven benefits, women are prescribed these therapies less frequently and are also less consistent in taking them. The result: women are, overall, more frequently undertreated.
Diabetes increases the risk of cardiovascular disease significantly more in women than in men: Women with diabetes have about a 7-fold increased risk, while for men it is about 3-fold.
The risk of coronary heart disease is also about 44 percent higher in women with diabetes than in men.
After menopause, women are more likely to develop a prediabetic condition (impaired glucose tolerance). This often goes unnoticed but already increases the risk of cardiovascular disease.
A special test (oral glucose tolerance test) can detect such early changes, allowing for timely intervention.
Why diabetes is particularly dangerous for women is not yet fully understood. Presumably, several factors play a role:
- more severe damage to blood vessels,
- increased blood clotting,
- frequent additional health conditions,
- and generally less frequent or less consistent treatment.
The good news: Modern diabetes medications such as GLP-1 agonists or SGLT2 inhibitors are equally effective in women and men.
It is therefore particularly important for women to detect diabetes early and treat it consistently in order to prevent cardiovascular disease.
Being overweight and obesity are particularly significant for women because they increase the risk of cardiovascular disease more than they do for men.
Studies show that obesity increases the risk of coronary heart disease by 64 percent in women and by 46 percent in men (Garcia et al. 2016).
After menopause, fat distribution in women also changes:
Fat is more likely to accumulate around the abdomen rather than on the hips and thighs. This so-called abdominal fat is particularly harmful because it is linked to elevated blood lipids, blood sugar problems, and metabolic syndrome.
Important: Waist circumference is a key risk factor for cardiovascular disease and life expectancy.
Guidelines for women:
- From 80 cm waist circumference: Maintain stable weight
- From 88 cm waist circumference: Weight loss recommended
In addition: Being overweight is one of the most important modifiable risk factors for high blood pressure in women.
Even small changes in weight—especially around the waist—can therefore significantly reduce heart disease risk.
A lack of exercise and an unhealthy diet increase the risk of cardiovascular disease in women—just as they do in men.
Conversely: Regular exercise and a balanced, heart-healthy diet significantly reduce the risk. An active lifestyle and a healthy diet are important building blocks for both genders in protecting the heart over the long term.
Large studies show that women who are active and eat a healthy diet are less likely to develop heart disease than men.
For example, an analysis of data from the UK Biobank (published in Nature Cardiovascular Research) shows that regular physical activity protects women more effectively against coronary heart disease than men: Participants who followed the exercise guidelines had a 22 percent lower risk of coronary heart disease among women and a 17 percent lower risk among men (Chen et al. 2025).
Another finding: With the same level of physical activity, women often achieve positive results faster than men. One study showed that men only saw a survival benefit starting at about 300 minutes of exercise per week, while women saw it as early as around 140 minutes.
Nevertheless, women—especially as they age—are often less physically active than men. They also participate less frequently in rehabilitation sports or structured exercise programs. Prevention and early intervention measures could be important levers for improving heart health in this context.
Although women smoke less frequently than men overall, smoking is particularly dangerous for them: Female smokers have a roughly 25 percent higher risk of heart attack than male smokers (Huyn et al. 2019). The number of female smokers has risen significantly in recent years.
Especially among younger women, smoking is the most important preventable risk factor for a severe heart attack (Gleerup et al. 2020).
The Nurses’ Health Study shows that coronary risk increases significantly with the number of cigarettes smoked per day:
- Former female smokers: approximately 1.5 times higher risk
- 1–14 cigarettes per day: approximately 3-fold increased risk
- More than 14 cigarettes per day: approximately 5.5-fold increased risk
The situation becomes particularly critical when combined with hormonal contraception such as the pill: The risk of a heart attack increases to 10 times, and the risk of stroke to 3 times (Geraghty et al. 2021).
E-cigarettes are also not a harmless alternative and can damage the cardiovascular system.
Quitting smoking is therefore one of the most important steps to effectively protect the heart—especially in younger women.
Specific risk factors for women
Certain conditions in which the immune system attacks the body’s own tissues occur significantly more frequently in women—for example, thyroid disorders or lupus (Cho et al. 2020).
These conditions are often accompanied by chronic inflammation throughout the body, which damages blood vessels and increases the risk of cardiovascular disease.
- In lupus patients, heart disease is actually the leading cause of death.
- In rheumatoid arthritisthe risk of dying from cardiovascular disease is increased by about 50 percent.
Symptoms (e.g., fatigue or shortness of breath) can also mask heart problems and make diagnosis difficult.
Effective treatment of the underlying disease and management of cardiovascular risk factors are therefore crucial.
Awareness of how much psychological stress affects heart health has grown significantly in recent years. This includes:
- depression and anxiety disorders
- traumatic experiences or violence
- chronic stress, social isolation, or financial worries
Psychosocial stress is now a recognized risk factor for cardiometabolic diseases.
Globally, women are nearly twice as likely as men to suffer from depression, which is associated with an increased risk of cardiovascular diseases such as coronary heart disease (Cho et al. 2020). It is unclear how high the number of undiagnosed cases of depression is among men. Due to sociocultural influences, stigmatization remains common, and there is concern that depression in men is therefore less frequently diagnosed and treated.
Socioeconomic disadvantage and often lower educational attainment are also risk factors for women’s heart health: they can contribute to lower health awareness, an unhealthy lifestyle, chronic stress, and depression (Busch & Kuhnert 2017).
More educational efforts, easier access to medical care, and greater social integration could help reduce the incidence of disease among women.
There is a close link between gynecological cancers and the development of cardiovascular diseases. Three examples:
Breast cancer is now increasingly treatable; many patients live significantly longer. However, this also makes the long-term effects of treatment more important. Especially after radiation therapy to the left breast, the risk of developing coronary heart disease may be increased. For this reason, special protective techniques are now used during radiation therapy to keep the radiation dose low.
Certain cancer treatments can lead to heart failure . These include chemotherapy or the use of certain medications.
Cardiac arrhythmias or high blood pressure can also develop as a result of cancer treatment, for example due to taking certain medications. This makes it all the more important to optimally control existing high blood pressure before starting cancer treatment and to closely monitor patients with normal blood pressure for any potential changes.
Learn more about the interdisciplinary treatment options at Charité
Pregnancy
Complications during pregnancy may indicate an increased risk of cardiovascular disease later in life:
- Repeated miscarriages or stillbirths increase the risk by 20–30 percent
- Also premature birth, low birth weight, and multiple births in a woman’s lifetime (multiparity) are risk factors for future heart disease
- Pregnancy-induced hypertension or preeclampsia significantly increases the risk of heart disease later in life. preeclampsia is a serious complication that occurs after the 20th week of pregnancy, characterized by high blood pressure and protein in the urine. It can lead to organ damage and often requires premature delivery. Symptoms include severe headaches, visual disturbances, and edema, such as in the hands, face, or feet.
- About one in two women with gestational diabetes later develops type 2 diabetes.
Regular follow-up visits and checkups are therefore particularly important after such pregnancies.
Breastfeeding for several months, on the other hand, can have a protective effect on the heart (Geraghty et al. 2021).
Menstrual cycle and PMS
Hormonal fluctuations during the cycle affect the heart and blood vessels. Women with premenstrual syndrome (PMS) sometimes experience increased heart palpitations, blood pressure fluctuations, or fatigue.
Over the long term, recurring hormonal stress can affect the cardiovascular system, especially when combined with other risk factors.
Cardiac arrhythmias occur more or less frequently in women depending on their cycle.
Hormonal disorders (e.g., PCOS)
Polycystic ovary syndrome (PCOS) is one of the most common hormonal disorders among women of childbearing age. In addition to menstrual irregularities or difficulty conceiving, PCOS often affects metabolism. Many affected women develop elevated blood sugar levels, high blood pressure, obesity, or unfavorable cholesterol and triglyceride levels.
These changes place a long-term strain on the heart and blood vessels. Studies therefore show that women with PCOS have a significantly increased risk of cardiovascular disease—the risk is about 40 percent higher than in women without PCOS. This makes early diagnosis, regular preventive care, and a conscious approach to potential risk factors all the more important.
Perimenopause, Menopause, and Early Menopause
Estrogen levels decline during menopause. This leads to increased cholesterol levels, changes in blood sugar metabolism, altered fat distribution (more abdominal fat), and higher blood pressure.
The result: Cardiovascular risk increases significantly.
An early menopause (before age 45) or very early hormonal decline (before age 40) further increase the risk—for every year of early menopause, the risk of cardiovascular disease rises by about 3 percent (Maas et al. 2021).
“Gender-specific cardiology is not a niche topic, but a central component of modern precision medicine. Our goal is to provide care that is personalized, scientifically sound, and interdisciplinary—for every patient.”
Prof. Dr. Ingo Hilgendorf
“Gender-specific cardiology is not a niche topic, but a central component of modern precision medicine. Our goal is to provide care that is personalized, scientifically sound, and interdisciplinary—for every patient.”
Prof. Dr. Ingo Hilgendorf
Cardiovascular Diseases: Gender Differences
Cardiovascular diseases are among the leading causes of death worldwide—yet they affect women and men differently. Gender-specific differences are evident in risk factors, symptoms, diagnosis, and treatment. While traditional research has long focused primarily on male patients, there is now an increasing recognition that women often exhibit different disease progression and warning signs. A better understanding of these differences is crucial for improving prevention, early detection, and treatment in a targeted manner and for optimizing healthcare for everyone. We outline some of the most important differences below.
Coronary heart disease (CHD)
In coronary heart disease, the coronary arteries—which supply the heart muscle with oxygen-rich blood—become calcified. If these calcifications cause narrowings or blockages, blood flow to the heart muscle is impeded accordingly. Significantly narrowed vessels can trigger a feeling of chest tightness (angina pectoris) during physical exertion. If a coronary vessel suddenly closes completely, a heart attack results.
On average, women develop the condition about 10 years laterthan men – presumably due, among other things, to hormonal protection in younger years. However, the risk increases significantly with age.
Why CHD is often diagnosed later in women
Women often have different changes in the coronary arteries than men: The vessels are not always severely narrowed, but rather diffusely affected. Often, the small vessels (microcirculation) are impaired. This means that even if the large vessels appear “normal,” there may still be a circulatory disorder in the heart.
Heart attacks in women
Overall, women have a poorer treatment outcome, primarily because:
- they often seek help later
- symptoms manifest differently
- diagnosis and treatment are delayed
Especially important:
- Younger women under 60 have a higher risk of dying in the hospital from a severe heart attack than men.
- There are specific types, such as the heart attack without narrowed vessels (myocardial infarction with non-obstructive coronary arteries MINOCA), which occur more frequently in women than in men.
Classic symptoms such as angina pectoris occur in 80 percent of heart attacks in both women and men.
However, women also more frequently report shortness of breath, nausea, or abdominal pain, as well as back or jaw pain, dizziness, weakness, or anxiety. These symptoms are often underestimated. This leads to delays—with consequences for treatment.
Diagnosis – more difficult in women
Many standard tests are less informative in women. Therefore, normal findings regarding the coronary arteries do not reliably rule out heart disease.
Further, more complex procedures are necessary to detect, for example, vascular spasms or microvascular dysfunction. It is particularly important to examine the small vessels, which are frequently affected in women.
Treatment
As a general rule: Women benefit just as much from therapies as men (e.g., stents, medications). However, women still receive these treatments less frequently than men and experience side effects such as bleeding more often. Even after procedures, women are more likely to have persistent symptoms because the small vessels are often additionally affected.
Especially important for women:
- Take symptoms seriously—even less common ones
- Seek medical evaluation early
- Consistently treat risk factors
Heart failure is a common condition that affects both women and men. In this condition, the heart is no longer able to supply the body with enough blood and oxygen.
Heart failure in women and men
Heart failure is one of the most common cardiovascular diseases in Germany and is a leading cause of hospitalizations and deaths. There are significant differences between the sexes:
- Women often develop heart failure only in later life. Men are affected earlier on average.
- The hormone estrogen protects the heart. Due to the decline in estrogen levels during menopause , the risk of cardiovascular disease increases in women. Women who experience early menopause (before age 40) have a higher risk of heart failure.
- Women are more likely to develop a form of heart failure in which pumping capacity appears normal, but the heart does not relax properly (heart failure with preserved ejection fraction HFpEF). Men, on the other hand, are more likely to develop heart failure with reduced ejection fraction (HFrEF).
- In addition to HFpEF, types of heart failure such as “broken heart syndrome” and peripartum cardiomyopathy occur more frequently or exclusively in women. “Broken heart syndrome” refers to a form of heart failure that occurs following highly emotional events and is particularly common in menopausal women. Peripartum cardiomyopathy is a form of heart failure that can occur during the last month of pregnancy or up to five months after childbirth.
- In addition, heart failure can be triggered by cancer treatment ,often, for example, following breast cancer therapy, which affects women in 99 percent of cases.
- In women, heart failure is diagnosed less frequently than in men.
- Since women are underrepresented in studies and guidelines, there is less data on optimal treatment.
- Women are admitted to the hospital for heart failure later and less frequently than men with heart failure.
- Men die more frequently from the consequences of heart failure as early as their younger and middle years. Women are more likely to have a poor quality of life.
- In cases of severe heart failure , women are less frequently referred to specialized clinics and are also less frequently and later placed on the waiting list for a heart transplant than men.
- Heart transplant recipients who wish to have children require close, interdisciplinary medical care before, after, and during childbirth.
Detailed information on gender-specific differences in heart failure, including references, is available in the Heart Atlas:
Cardiac arrhythmias occur when the heart’s electrical system becomes unbalanced. The heart then beats too fast, too slow, or irregularly. Gender-specific differences play an important role here: Women and men differ not only in symptoms and disease prevalence, but also in how medications work and the success of certain therapies.
Even the electrical activity of a healthy heart differs between women and men. Hormones such as estrogen, progesterone, and testosterone influence the electrical properties of heart muscle cells and thus the heart rhythm. For example, women’s heart rate is usually slightly faster, while the heart’s so-called electrical recovery phase—the QT interval on the ECG—is naturally longer than in men. These differences primarily emerge during puberty and also change throughout the menstrual cycle, during pregnancy, and during menopause.
As a result, women are more sensitive to certain arrhythmias and to medications that affect heart rhythm. The so-called long-QT syndrome is particularly relevant. In this condition, the heart’s electrical recovery phase is prolonged, which can trigger dangerous arrhythmias.
Women have an increased risk of so-called Torsade de Pointes tachycardias—potentially life-threatening arrhythmias that can be triggered by certain antibiotics, psychotropic drugs, or heart medications, among other factors. Therefore, medications and dosages must be evaluated with particular care in women (Vogel et al. 2021).
Hormonal changes can also influence the risk of cardiac arrhythmias. During pregnancy, the postpartum period, or menopause, the heart’s electrical stability changes. Particularly in the first few months after childbirth, the risk of certain arrhythmias may be temporarily elevated. At the same time, congenital forms of long QT syndrome are more common in women and sometimes present differently than in men.
One of the most common cardiac arrhythmias is atrial fibrillation. Women usually develop it at an older age and are more likely to have comorbidities such as high blood pressure or heart failure. Many female patients report heart palpitations, shortness of breath, dizziness, restlessness, or severe fatigue. These symptoms often affect women more severely than men. At the same time, their risk of stroke is increased. For this reason, current guidelines often recommend early anticoagulation for women with atrial fibrillation to prevent strokes (Hindricks et al. 2021).
Despite more severe symptoms, women are less likely to receive appropriate treatments such as catheter ablation or electrical cardioversion(Etaee et al. 2021). At the same time, side effects occur more frequently with drug therapies. Studies also show that women are more likely to develop atrial fibrillation again after ablation. Reasons for this include structural changes in heart tissue and different electrical triggers of the arrhythmia.
Other supraventricular arrhythmias also occur more frequently in women. These include, in particular, atrioventricular nodal reentry tachycardia (AVNRT), a form of sudden-onset rapid heartbeat. Hormonal fluctuations can influence the frequency of these symptoms. Overall, women report a reduced quality of life due to cardiac arrhythmias more frequently than men.
Severe ventricular arrhythmias and sudden cardiac death, on the other hand, occur less frequently overall in women than in men. When they do occur, women are usually older and more often have a structurally healthy heart. Nevertheless, individual risks must be carefully assessed—especially in cases of hereditary arrhythmias or a family history of the condition.
Heart valve diseases affect women and men differently. Differences are evident not only in the prevalence of certain conditions, but also in symptoms, disease progression, diagnosis, and treatment outcomes.
Many of today’s threshold values and surgical criteria were originally developed primarily based on male patient groups. As a result, heart valve diseases in women are often detected later or treated only at an advanced stage.
Women also often have different anatomical conditions than men. Heart valves and blood vessels are usually smaller, which can make procedures more technically challenging and increase the risk of complications. For this reason, professional societies such as the American Society of Echocardiography now recommend assessing heart size and heart function on a gender-specific basis and adjusting these measurements more closely to body surface area (Youssef 2021).
The most common heart valve disease in older adults is aortic valve stenosis – a narrowing of the aortic valve. Women usually develop the condition at an older age than men and are more likely to exhibit degenerative changes in the valve. Although valve calcification is often less pronounced, the heart in women reacts differently to chronic stress: The heart wall thickens more significantly and the ventricle remains smaller. After successful treatment, this change often regresses more quickly in women.
With traditional surgical aortic valve replacement, women have a higher overall risk of complications. One reason for this is the smaller anatomy of the heart valve, which means that implanted prosthetic valves sometimes do not fit the patient’s body size optimally. The situation is different with catheter-based aortic valve implantation (TAVI). Here, despite slightly more frequent procedural complications, women overall show better long-term outcomes than men. Studies indicate that women can particularly benefit from this less invasive procedure.
Diseases of the mitral valve also differ between the sexes. Women are more likely to have certain forms of mitral valve prolapse—a condition affecting the heart valve between the left atrium and the left ventricle. Rheumatic mitral valve disease is also more common in women. At the same time, female patients often experience more severe symptoms but undergo surgery less frequently and at a later stage than men. As a result, treatment often does not occur until the disease has reached an advanced stage.
Modern catheter-based procedures for treating the mitral valve, such as so-called “edge-to-edge” repairs, show results in women that are comparable to those in men. Nevertheless, the risk of readmission to the hospital due to heart failure remains elevated in many female patients.
Diseases of the tricuspid valve also predominantly affect women. These are often a consequence of other heart or lung diseases that place a strain on the right ventricle. Catheter-based therapies are becoming increasingly important in this context, and gender-specific differences are currently being intensively studied.
Congenital heart defectsalso show differences between women and men. Some malformations are more common in men, while other conditions progress differently in women or are associated with an increased risk of complications such as pulmonary hypertension. Thanks to modern diagnostics and specialized care, many patients with congenital heart defects now reach adulthood and require long-term interdisciplinary care.
Pulmonary hypertension is a condition in which blood pressure in the pulmonary vessels is chronically elevated. This places a particularly heavy strain on the right side of the heart. The condition can lead to shortness of breath, reduced exercise tolerance, fatigue, dizziness, or heart failure.
Women are significantly more likely to be affected by pulmonary hypertension than men. Depending on the form of the disease, the proportion of women in large international registries ranges between 65 and 80 percent (Oakland and Joseph 2021).
Reasons for this include hormonal and genetic differences. In particular, the female sex hormone estrogen and its metabolites appear to play an important role in the development of the disease. Certain genetic variations, which increase the risk of pulmonary hypertension, also manifest more frequently in women with clinical consequences.
Despite the higher risk of developing the disease, women with pulmonary hypertension often have a better prognosis than men. Experts refer to this as the so-called “estrogen paradox.” Studies show that women often have better function of the right ventricle—that is, the half of the heart that must work against the increased pressure in the lungs. As a result, the disease progresses more slowly in many female patients, and the overall survival rate is higher (Oakland and Joseph 2021).
Women with pulmonary hypertension often have more favorable hemodynamic conditions: The right ventricle can often continue to pump adequately for longer despite the increased pressure load. This is considered a key reason for the often more favorable disease course.
Gender-specific differences in drug therapy have not yet been conclusively demonstrated. Nevertheless, individualized care is particularly important, as symptoms, exercise tolerance, and disease progression can vary greatly.
The condition is of particular significance during pregnancy. Women with pulmonary hypertension face a significantly increased risk of severe complications during pregnancy and childbirth. The additional strain on the heart and lungs can become life-threatening. Therefore, international guidelines recommend avoiding pregnancy in cases of pulmonary hypertension whenever possible, or assessing the risks early on through an interdisciplinary approach and providing long-term interdisciplinary care for patients (Regitz-Zagrosek et al. 2018).
A pulmonary embolism occurs when a blood clot blocks a blood vessel in the lung. This clot usually originates in the veins of the legs or pelvis and is carried to the lungs via the bloodstream. The condition can occur suddenly and lead to shortness of breath, chest pain, rapid heartbeat, dizziness, or circulatory problems. Women and men are affected with similar frequency overall – however, there are significant differences depending on age and hormonal status.
Between the ages of 20 and 40, women suffer from pulmonary embolism significantly more often than men. Hormonal influences are primarily responsible for this. In particular, estrogen-containing contraceptives as well as hormonal therapies during menopause increase the risk of blood clots. Pregnancy and the postpartum period are also considered significant risk phases. In older age, however, the incidence of pulmonary embolism increases more sharply in men.
Women often exhibit more pronounced symptoms of pulmonary embolism – both during the acute phase and in the long term. Many patients report severe shortness of breath, exhaustion, or a prolonged reduction in physical capacity. At the same time, the symptoms can be nonspecific and initially attributed to other causes.
Standardized risk assessments and blood tests are used for diagnosis. The so-called D-dimer level plays an important role in this context. This blood value is often naturally higher in women than in men—especially during hormone therapy. Therefore, there is ongoing discussion about whether gender-specific threshold values could improve diagnosis in the future. Imaging techniques such as CT pulmonary angiography are considered particularly reliable in women (Jarman et al. 2021).
In the treatment of pulmonary embolism, blood-thinning medications are used to prevent further clots. Modern oral anticoagulants (NOACs) are just as effective in women as they are in men. At the same time, women on anticoagulation or thrombolytic therapy experience clinically significant bleeding more frequently. In younger female patients, heavy menstrual bleeding in particular can be an additional burden when taking blood-thinning medication. Therefore, individually tailored treatment is especially important.
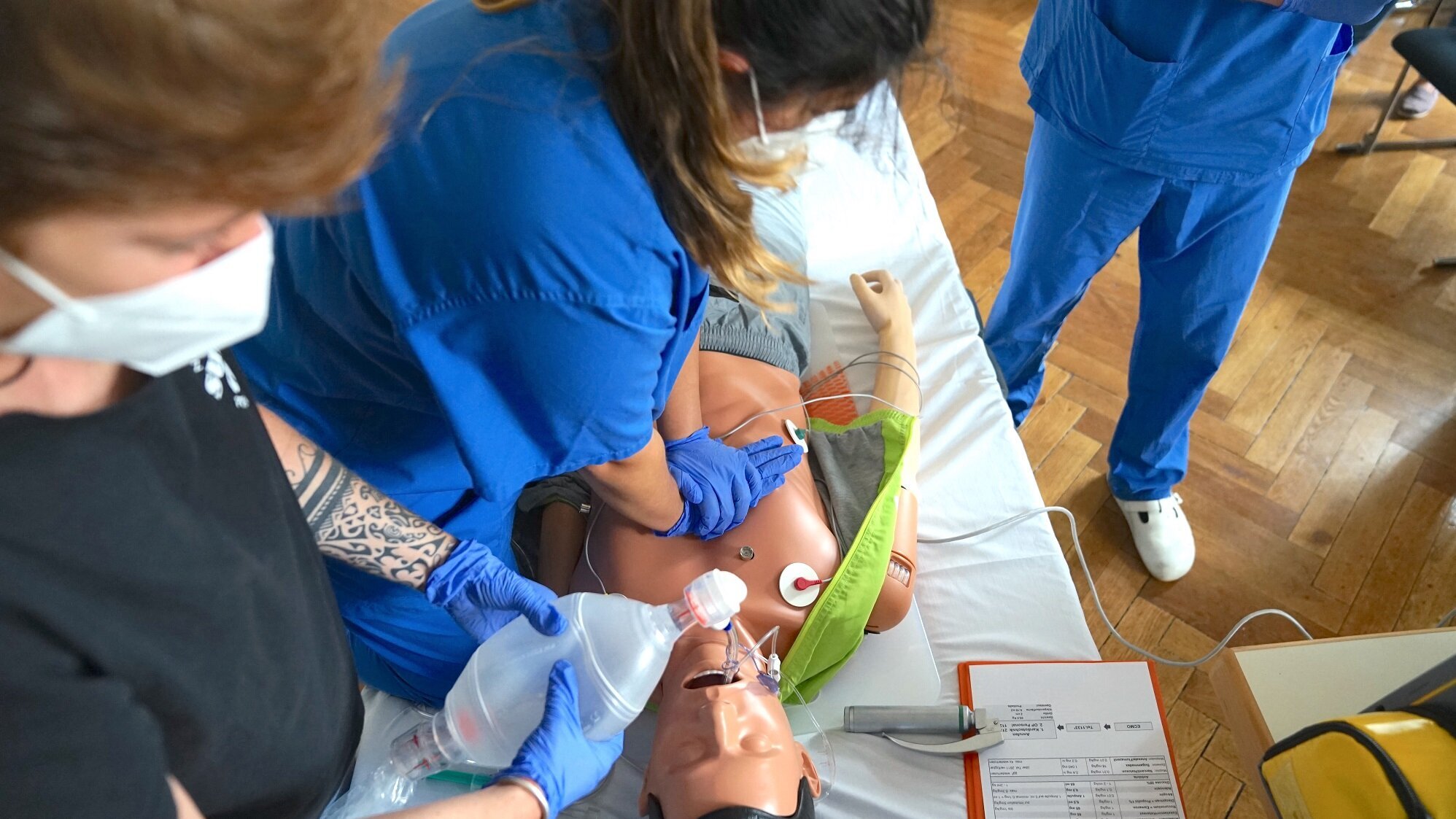
Topic: Resuscitation
Women are less likely to receive CPR than men when they suffer a cardiac arrest in public.
The reasons for this do not lie in the condition itself—but in uncertainty, prejudice, and false assumptions.
Yet the most important rule is simple:
Don’t wait. Press.
Women are less likely to receive CPR than men when they suffer a cardiac arrest in public.
The reasons for this do not lie in the condition itself—but in uncertainty, prejudice, and false assumptions.
Yet the most important rule is simple:
Don’t wait. Press.
Topic: Medication Dosage
Same dose – different effect: Many medications have been tested primarily on men. As a result, standard dosages are often prescribed for everyone—even though women and men differ biologically. This can lead to womenreacting differently to the same dose.

Same dose – different effect: Many medications have been tested primarily on men. As a result, standard dosages are often prescribed for everyone—even though women and men differ biologically. This can lead to womenreacting differently to the same dose.
Topic: Heart Attack
Heart attack symptoms in women are still often described as “atypical.” The problem is that “atypical” sounds vague, less clear-cut—perhaps even less urgent.
One thing is clear: A heart attack does not have to fit the classic profile to be a medical emergency.

Heart attack symptoms in women are still often described as “atypical.” The problem is that “atypical” sounds vague, less clear-cut—perhaps even less urgent.
One thing is clear: A heart attack does not have to fit the classic profile to be a medical emergency.
Topic: High-Risk Pregnancy
Vivien F., 33, was suddenly diagnosed with “idiopathic pulmonary hypertension.” Despite the increased risk, she and her partner Benedikt made a conscious decision to have a child. During her pregnancy, she received interdisciplinary care at the DHZC and Charité, and gave birth to her son at the end of April.

Vivien F., 33, was suddenly diagnosed with “idiopathic pulmonary hypertension.” Despite the increased risk, she and her partner Benedikt made a conscious decision to have a child. During her pregnancy, she received interdisciplinary care at the DHZC and Charité, and gave birth to her son at the end of April.
Our Expertise at the DHZC | Diagnostics, Counseling & Treatment
Cardiovascular diseases are the leading cause of death among both women and men; however, there are many gender-specific characteristics. These differences must be taken into account in risk stratification, diagnosis, and treatment. Pregnancy and menopause represent two unique phases of life for women during which cardiovascular diseases may first occur or undergo significant changes.
Our specialized women’s heart clinic offers women with increased cardiovascular risk as well as known heart disease individualized cardiological care with a special focus on pregnancy and (peri-)menopause.
Our Areas of Focus:
- Cardiovascular Risk Management for Women
- Cardiological Care Before, During, and After Pregnancy for Patients with Pre-existing Heart Conditions
- High blood pressure, preeclampsia, cardiomyopathies, and heart failure during pregnancy
- Cardiac arrhythmias during pregnancy
- Management of cardiovascular risk factors during (peri-)menopause
- Interdisciplinary care in close collaboration with nephrology, obstetrics, and gynecology
In a monthly Pregnancy Heart Team, high-risk cardiovascular patients during pregnancy are discussed in an interdisciplinary setting with colleagues from cardiology, obstetrics, and anesthesiology across campuses, and treatment plans are established before, during, and after delivery.
Women with congenital heart defects are cared for in our certified EMAH Center – including during pregnancy.
Office hours: Tuesday 8:00 − 2:00 p.m.
Contact person: Dr. Julia Lueg
At our gynecological heart health clinic, we care for women who are at increased risk for cardiovascular disease or who wish to specifically improve their heart health. We also care for pregnant women who have existing heart or circulatory conditions or are at increased risk for them.
Our goal is to provide the best possible support during pregnancy, prevent complications, and protect your heart health in the long term.
KIM Address for Referring Physicians: hochrisiko-cvk@dhzc-charite.kim.telematik
Head of the Clinic: PD Dr. med. Kun Zhang
Interdisciplinary collaboration
The Cardiogenetics Clinic at the Department of Cardiology, Angiology, and Intensive Care Medicine at the CCM focuses on the diagnosis and treatment of inherited cardiac arrhythmias and heart muscle diseases. In addition, it provides care for patients who have survived unexplained sudden cardiac death, as well as their families.
There is close collaboration with the Clinic for Women with Heart Disease at the CCM as well as with the Department of Obstetrics at Charité. The goal of this interdisciplinary treatment is to provide holistic and personalized care for patients.
Our Services
For pregnant women with cardiovascular diseases or suspected cardiovascular conditions, a precise risk assessment (risk stratification) is particularly important to ensure the best possible care for both the expectant mother and the unborn child. In addition to cardiological and obstetric care, cardiogenetics also plays an important role: It supports the diagnosis of the condition and involves the entire family in the diagnostic process and counseling.
We therefore offer pregnant women with existing or suspected cardiovascular disease an evaluation to determine whether a hereditary heart condition is present. In this context, we also discuss the underlying genetic causes and assess the risk of transmission to future generations. This helps determine whether genetic testing of other family members—especially the child—is advisable.
“Genetic heart diseases can become apparent for the first time during pregnancy. At the same time, this is a particularly sensitive phase of life with an increased risk of transmission to the unborn child. We always consider genetic diseases in the context of the entire family, thereby closing an important gap in care,” says Prof. Wilhelm Haverkamp, head of the clinic.
The interplay of cardiogenetics and clinical care lays the foundation for modern precision medicine and enables individualized prevention and treatment. This is particularly important in the case of inherited diseases as well as during sensitive life stages such as pregnancy or menopause.
Head of the clinic: Prof. Dr. Wilhelm Haverkamp
The Pregnancy Heart Team cares for patients with pre-existing cardiovascular conditions as well as pregnancy-related cardiovascular diseases during pregnancy and facilitates proactive, interdisciplinary birth planning that consistently takes individual needs into account.
Through an interdisciplinary team of specialists in cardiology, pediatric cardiology, and anesthesia at the DHZC, as well as obstetrics at Charité, we ensure close and individually tailored care.
In monthly case conferences, experts from the aforementioned disciplines come together to determine the treatment and care of high-risk cardiovascular patients during pregnancy, before, during, and after childbirth.
This close interdisciplinary collaboration forms the basis for optimal, individually tailored, and long-term care for our patients.
Director: Dr. Teresa Mira Gruber, M.D., Senior Physician at the Department of Obstetrics at Charité
Causes, symptoms, and effects of the condition
Preeclampsia affects approximately two to eight percent of all pregnant women and is one of the most common causes of preterm birth worldwide, as well as serious complications during pregnancy and childbirth.
Clinically, the condition is primarily characterized by high blood pressure, often in combination with further organ damage. The kidneys are particularly often affected, so that increased protein excretion in the urine may be detectable.
Typical symptoms experienced by those affected include headaches, visual disturbances, increasing fluid retention, nausea, or pain in the upper abdomen. The unborn child may also be affected: restricted blood supply via the placenta can lead to growth disorders, which in severe cases may necessitate premature birth.
The causes of preeclampsia are not yet fully understood. A key factor is believed to be abnormal development of the placenta in early pregnancy. This leads to pathological changes in the blood vessels as well as inflammatory reactions throughout the body. Vascular-damaging signaling molecules produced in the placenta play a particular role; these can now be measured in the blood as biomarkers.
If left untreated, preeclampsia can have serious health consequences for both mother and child. Furthermore, affected women face an increased long-term risk of cardiovascular and kidney diseases. Regular prenatal checkups during pregnancy as well as consistent postnatal care after childbirth are therefore of great importance.
Interdisciplinary treatment at Charité
Preeclampsia can occur in women with or without pre-existing conditions. However, pregnant women with underlying internal medical conditions are particularly frequently affected. At the same time, women who have had preeclampsia have an increased risk of subsequent cardiovascular or kidney damage.
The prevention, treatment, and long-term care of these patients therefore require close collaboration among highly specialized departments. The Preeclampsia Working Group at the Department of Obstetrics at Charité serves as a central hub for this purpose, linking prenatal care, acute care, and long-term follow-up.
The working group’s goal is to gain a better scientific understanding of the causes of the disease while simultaneously improving the interdisciplinary care of patients and their children in the long term.
To this end, specialists at Charité conduct basic research on the development of the diseased placenta, develop clinical algorithms and predictive models for optimized management of the disease, and provide treatment in accordance with current international standards.
This involves close collaboration with colleagues in cardiology, angiology, and intensive care medicine at the DHZC as well as with the Department of Nephrology at Charité.
Since high blood pressure, vascular damage, and kidney disease associated with preeclampsia significantly increase the risk of later cardiovascular disease and permanent kidney damage, high-risk patients in obstetrics are informed, educated, and provided with long-term follow-up care through the specialized clinics at the DHZC. There is close collaboration with and follow-up care provided by:
- Dr. Julia Lueg (Charité Mitte Campus)
- PD Dr. Kun Zhang (Virchow-Klinikum Campus)
- Dr. Evelyn Seelow (Department of Nephrology, Charité Mitte Campus)
- Dr. Julia Seelemann (Department of Nephrology, Virchow-Klinikum Campus)
In collaboration with the Department of Cardiology, the Friede Springer Cardiovascular Prevention Center and the Experimental and Clinical Research Center (ECRC) at Charité, interdisciplinary collaboration within the Preeclampsia Working Group is to be further expanded. PD Dr. Ralf Dechend (ECRC) and Prof. Dr. Elisabeth Steinhagen-Thiessen (Friede Springer Cardiovascular Prevention Center).
Further information on the Preeclampsia Working Group
Leadership: Dr. Lisa Antonia Lorenz-Meyer, Senior Physician at the Department of Obstetrics at Charité
The Survivorship Clinic at Charité is dedicated to improving care for long-term survivors of gynecological cancer. The clinic is intended for patients who have been diagnosed with ovarian, fallopian tube, or peritoneal cancer; endometrial cancer; cervical cancer; vaginal cancer; or breast cancer, and whose initial diagnosis occurred at least five years ago—regardless of their current health status.
During the clinic , patients receive counseling on long-term side effects, tumor follow-up care, and health-promoting measures. In addition, an individualized prevention and treatment plan (Survivorship Care Plan) is developed together.
Close collaboration with the DHZC Cardiology Department
There is a close link between gynecological cancers and the development of cardiovascular diseases.
Many patients already have cardiovascular risk factors such as high blood pressure, diabetes, or obesity before starting cancer treatment, which can further increase the risk of subsequent cardiovascular diseases. At the same time, oncological therapies themselves can have cardiotoxic effects and cause, among other things, heart failure, coronary heart disease, cardiac arrhythmias, or treatment-associated hypertension.
With rising survival rates, therefore, in addition to tumor therapy, long-term cardiovascular care is becoming increasingly important. Secondary and tertiary prevention play a central role in this context: The goal is to treat existing risk factors early on, detect treatment-related heart damage in a timely manner, and sustainably reduce the long-term increased cardiovascular risk following a cancer diagnosis.
For this reason, patients treated in the Charité’s survivorship clinic are referred to the DHZC’s specialized clinics for further evaluation if they present a corresponding risk profile. This ensures early diagnosis and long-term management of cardiovascular diseases.
Head of the Clinic: PD Dr. Hannah Woopen, MSc
Director of the Charité Clinic for Gynecology (CVK): Prof. Dr. Jalid Sehouli
“Long-term cardiovascular effects are not a problem limited to specific types of cancer, but affect women with nearly all types of cancer.”
PD Dr. Hannah Woopen

“Long-term cardiovascular effects are not a problem limited to specific types of cancer, but affect women with nearly all types of cancer.”
PD Dr. Hannah Woopen
“Collaboration between gynecology, oncology, cardiology, and other specialties is essential for providing patients with comprehensive care and targeted treatment. Looking at just one organ in isolation is not enough.”
Prof. Dr. Jalid Sehouli
“Collaboration between gynecology, oncology, cardiology, and other specialties is essential for providing patients with comprehensive care and targeted treatment. Looking at just one organ in isolation is not enough.”
Prof. Dr. Jalid Sehouli
Research on gender-specific cardiology
At the DHZC, we conduct extensive research on gender-specific differences in cardiology. Our goal is to better understand why cardiovascular diseases progress differently in women and men—from risk factors and symptoms to treatment outcomes. The following selected projects and publications provide insights into relevant scientific literature, current research approaches, and potential innovative treatment strategies.
Selected Research Projects & Publications
MINOCA: Gender-specific causes & personalized treatments for the “silent heart attack”
A heart attack is usually associated with blocked coronary arteries. However, not all patients exhibit such typical blockages. In the case of a heart attack without narrowed coronary arteries, known as MINOCA (myocardial infarction with non-obstructive coronary arteries), narrowing and circulatory disturbances can also occur—though often in the smaller vessels of the heart rather than in the major coronary arteries. As a result, these changes often remain undetected in standard examinations. To detect these so-called microinfarcts , highly sensitive diagnostic procedures such as cardiac MRI are necessary.
MINOCA is not a single disease, but a collective term for various causes—including vasospasm, spontaneous coronary artery dissection, small blood clots, or disorders of the smallest heart vessels.
At the DHZC, a specialized cardiac surgery research group is investigating why MINOCA manifests differently in women and men and how diagnosis and treatment can be improved.
This specific type of heart attack accounts for about ten percent of all heart attacks and affects women more frequently than men in some forms of the disease. For example, spontaneous vessel wall tears or microvascular dysfunction occur more often in women than in men.
Reasons for the gender-specific differences
The researchers assume that, in addition to classic risk factors for a heart attack such as smoking, high blood pressure, or diabetes, gender-specific factors also play an important role in the development of MINOCA. These include complications during pregnancy, preeclampsia, hormonal changes during menopause, or autoimmune diseases, which are more common in women than in men. For a long time, many of these factors were rarely recorded or evaluated in cardiac research.
“Data on patients’ menstrual cycles, medication, and medical history—such as complications during pregnancy—have only recently begun to be systematically recorded and included in scientific analyses,” says Dr. Chistien Beez, who conducts research on the topic as the scientific director in the working group led by Prof. Maximilian Emmert.
Heart Failure in Women: Reliably Diagnosing and Treating Tricuspid Valve Insufficiency
A recent study by DHZC cardiologists Dr. Isabel Mattig (first author) and Prof. Dr. Henryk Dreger (last author) shows: Women with heart failure are significantly more likely to be affected by moderate-to-severe tricuspid valve regurgitation than men. This leakage of the heart valve between the right atrium and the right ventricle worsens the prognosis for patients. The DHZC study demonstrates for the first time clear differences between the sexes and the forms of heart failure.
The results show that in women, tricuspid valve regurgitation worsens the prognosis particularly when heart failure is accompanied by preserved ejection fraction. In men, on the other hand, tricuspid valve regurgitation is particularly dangerous when heart failure is accompanied by reduced pumping power .
Why women are more likely to develop HFpEF than men
Heart failure is not always the same: Women particularly often develop a form of heart failure in which the heart’s pumping power is preserved, but the heart can no longer relax and fill sufficiently. Experts refer to this as heart failure with preserved ejection fraction (HFpEF). Especially after menopause, women are affected significantly more often than men.
Researchers at Charité are investigating, within the DFG Collaborative Research Center 1470, the role that sex hormones, the immune system, and the gut microbiome play in this form of heart failure.
The research focuses on the question of why hormonal changes—such as those during menopause—can influence inflammatory processes, metabolism, and the small blood vessels of the heart. The researchers suspect that changes in the gut microbiome and the immune system contribute to reduced blood flow in the fine heart vessels and changes in heart tissue. This can lead to heart failure in the long term.
To better understand these connections, state-of-the-art “multi-omics” methods are being used. In this process, the scientists simultaneously analyze genetic, immunological, microbiological, and metabolic data from experimental models and patient cohorts. The goal is to better identify gender-specific mechanisms of heart failure and to develop new, individually tailored therapies.
Research shows that gender-specific differences affect not only symptoms and disease progression but also extend to the biological foundations of cardiovascular diseases. It is precisely this understanding that is crucial for more precise and equitable cardiology.
Diagnosis and Treatment of Myocarditis: Why Age and Gender Matter
A recent study led by DHZC cardiologists Dr. Tharusan Thevathasan (first author) and Prof. Dr. Bettina Heidecker (corresponding author) shows that myocarditis (myocarditis) progresses very differently depending on age and gender. For clinical care, this means that patients require individually tailored diagnosis and treatment.
What does this mean for patients?
The study highlights three key points:
- Young men (especially between puberty and age 35) develop myocarditis significantly more frequently.
- Children (under 11 years old for girls and under 13 years old for boys) as well as older adults (54 years and older) have the highest risk of severe disease and a higher risk of death.
- As people age, the differences between women and men even out. In this age group, nearly as many women as men develop myocarditis.
This means: Age and gender provide important clues about how the disease will progress and how intensively it needs to be treated.
Severeaortic valve stenosis is one of the most common heart valve diseases in older adults. Today, the narrowed heart valve can be either surgically replaced or treated using a catheter-based procedure—known as transcatheter aortic valve implantation (TAVI). Researchers from the DEDICATE-DZHK6 study have investigated whether women and men benefit differently from these procedures.
Approximately 100 cardiac centers are participating in the study, including researchers from the DHZC: among others, Prof. Volkmar Falk,Prof. Ulf Landmesser and Prof. Henryk Dreger. The data from nearly 1,400 patients with severe aortic valve stenosis were analyzed.
The results show clear gender-specific differences: Women were older on average at the time of treatment and, despite having fewer comorbidities overall, had a higher surgical risk than men. At the same time, women benefited particularly strongly from catheter-based treatment (TAVI): After one year, they experienced strokes or deaths less frequently than after surgical valve replacement.
At the same time, the study showed that women developed early complications more frequently, regardless of the procedure chosen. After surgery, their risk of stroke was elevated. Men, on the other hand, were more likely to have comorbidities such as diabetes, coronary heart disease, or atrial fibrillation.
The research makes it clear that women and men have different risks and disease courses when it comes to heart valve disease. These differences should be taken into account more strongly in future treatment decisions. The goal is more personalized cardiac medicine, in which treatment methods are better adapted to biological and gender-specific characteristics.
TAVI Study: Women Experience More Stress Before and After the Procedure—and Require Tailored Care
Psychosocial Support Services and Close Monitoring Can Improve Treatment Outcomes
Transcatheter aortic valve implantation (TAVI) is an established, minimally invasive procedure for treating a narrowed aortic valve. How do women and men feel before and after the procedure, and what are the implications for treatment? DHZC researchers investigated this question in a study. They identified clear gender-specific differences—women were more anxious than men before the procedure and also experienced symptoms more frequently after TAVI: They stayed in the hospital longer, had greater difficulty with everyday tasks such as walking and shopping, felt more helpless, and exhibited increased depressive symptoms.
The results highlight the importance of individualized care. “Our analyses show that women often need tailored support services around TAVI that differ from those for men. Greater attention to post-operative care and targeted psychological support—both before and after the procedure—can help reduce anxiety and provide a greater sense of security. These differences should be given greater consideration in everyday clinical practice,” says Dr. Tharusan Thevathasan, a physician and researcher at the Department of Cardiology, Angiology, and Intensive Care Medicine at the Benjamin Franklin Campus and lead author of the study.
Differences in Survival Rates Following Cardiac Arrest
A cardiac arrest is a medical emergency in which every minute counts. Despite major advances in emergency and intensive care medicine, many people still die from the consequences of cardiac arrest. Researchers at the DHZC have therefore investigated how survival rates, treatment, and hospital care have changed in recent years—and what differences exist between different patient groups.
Among those involved in the study were Dr. Tharusan Thevathasan (first author), Prof. Carsten Skurk (last author), Prof. Ulf Landmesser, Dr. Wulf Knie and Dr. Georg Girke. The analysis was based on data from nearly 250,000 patients in the U.S. over a ten-year period.
The results show: The chances of survival after cardiac arrest have improved in recent years. At the same time, hospital stays became shorter, while modern intensive care therapies—such as mechanical circulatory support systems—were used more frequently.
However, differences between individual population groups were particularly striking. Older people, non-white patients, and those with severe illnesses had a significantly higher risk of death. In addition, the number of young adults experiencing cardiac arrest increased significantly during the study period.
The study highlights the importance of personalized cardiac care. Gender, age, pre-existing conditions, and social factors can have a decisive influence on how well people are treated after cardiac arrest and what their chances of survival are. The goal of the research is therefore to better understand differences in care and to further improve treatment for all patients.
Stroke Prevention Procedures: Gender-Specific Differences
Atrial fibrillation is one of the most common cardiac arrhythmias and significantly increases the risk of stroke. For patients who cannot take blood-thinning medications, closure of the so-called left atrial appendage (Left Atrial Appendage Closure, LAAC) can be an important alternative. This procedure involves inserting a so-called occluder, a small implant designed to prevent blood clots from forming and reaching the brain.
Researchers at the DHZC, together with international partners, investigated how safe this procedure is in everyday clinical practice—and what differences exist between women and men. Among those involved were Dr. Tharusan Thevathasan (first author), Prof. Carsten Skurk (corresponding author), Prof. Ulf Landmesser, Prof. Philipp Attanasio, Dr. Markus Reinthaler and Dr. Patrick Nagel.
Data from more than 11,000 patients in the U.S. were analyzed for the study. The results show that the procedure has become significantly safer overall in recent years. Complications occurred less frequently, hospital stays were shorter, and treatment could be performed more efficiently.
At the same time, the study revealed important gender-specific differences: Women had a higher risk of certain complications after the procedure, such as fluid buildup around the heart or vascular occlusions caused by blood clots. Additionally, regional differences in care for women and men were observed.
The study underscores the importance of gender-sensitive cardiology. Differences between women and men must be taken into account more closely to make procedures even safer and tailor treatments more individually.
Atrial Fibrillation: Why Gender-Specific Data Is Important Even in Catheter Ablation
Atrial fibrillation is the most common persistent cardiac arrhythmia and does not always affect women and men in the same way. Women are often older at the time of treatment, have different comorbidities, and may also differ from male patients in terms of anatomy, risk profile, and disease progression. Nevertheless, many technical ablation strategies and analyses are still based primarily on data that take gender-specific differences into account only to a limited extent.
Researchers at the German Heart Center at Charité are therefore investigating whether gender-specific patterns can be identified in the ablation of atrial fibrillation. In this treatment, specific areas of the heart muscle near the pulmonary veins are ablated to interrupt abnormal electrical impulses that can trigger or sustain atrial fibrillation.
The current analysis focuses on the question of whether women and men receive a comparable dose during ablation—and whether technical treatment parameters are associated with the subsequent recurrence of arrhythmias. Initial evaluations of more than 2,000 treatments suggest that women in the study group were more likely to experience a recurrence of arrhythmias within twelve months. At the same time, there were indications that a lower dose could be associated with a higher risk of recurrence.
What is particularly relevant here is not only whether an ablation is performed, but how the energy is delivered to the tissue. To this end, the researchers analyze time-dependent temperature curves during the ablation and additionally use machine learning methods. This allows them to identify complex patterns that might be overlooked with traditional single parameters.
The goal of the project is to better understand whether women might require different technical conditions or adjustments for certain ablation procedures than men. No immediate treatment recommendations can be derived from this yet; however, the data already show why gender-specific cardiology begins not only with symptoms, risk factors, or medication dosages, but also with interventional procedures and their technical details.
The research makes it clear: more precise cardiology means systematically capturing differences rather than explaining them after the fact. Especially for common conditions such as atrial fibrillation, this can help in the long term to plan treatments, better predict relapses, and tailor care for women and men more individually.
Scientific contacts at the DHZC are Prof. Dr. Felix Hohendanner and Dr. Emanuel Heil.
Study Examines Link Between Hormone Therapies & Atherosclerosis
Atherosclerosis, colloquially known as “hardening of the arteries,” refers to a chronic disease of the blood vessels in which deposits form in the arteries. As a result, the vessels lose elasticity and narrow, which increases the risk of heart attack, stroke, and other cardiovascular diseases.
The research project “Impact of new Hormone Replacement Therapy Delivery Methods on Cardiovascular Risk in High-Risk Postmenopausal Women” examines the influence of modern forms of hormone therapy during menopause on the development and progression of atherosclerosis as well as on cardiovascular risk in women. The focus is on new forms of hormone therapy delivery, such as creams, gels, or sprays, which may have beneficial effects on blood vessels and metabolism.
The prospective long-term study includes peri- and postmenopausal women with elevated cardiovascular risk, including women with existing cardiovascular disease or an elevated SCORE2 risk. The SCORE2 risk score describes the probability of experiencing a serious cardiovascular event, such as a heart attack or stroke, within the next ten years. The calculation is based, among other factors, on age, blood pressure, cholesterol levels, and smoking status.
The study will monitor whether participants are already receiving hormone therapy or not—the decision regarding therapy is made independently of the study and is not influenced by the study team.
Over a period of up to ten years, clinical events, risk factors, laboratory values, lifestyle factors, and changes in vascular health will be recorded. In addition, blood samples are stored for analysis of hormones and inflammatory markers. The goal is to gain new insights into whether modern hormone therapies can positively influence the progression of atherosclerosis and associated cardiovascular diseases.
The scientific contact person at the DHZC is Dr. Julia Lueg.
Gender-Sensitive Diagnostics in Echocardiography
Women and men differ not only in terms of symptoms and disease progression, but also in the structure and function of the heart. That is why gender-specific reference values play an important role in echocardiography – the ultrasound examination of the heart. Only when these differences are taken into account can heart diseases be accurately detected and correctly classified.
At the DHZC, an interdisciplinary team is working to further personalize echocardiography findings. Among those involved are Dr. Ursula Wilkenshoff,Dr. Anna Sannino, Dr. Elena Romero Dorta, uid=1136">Dr. Nikolas Merke and Dr. Matthias Schneider-Reigbert. Together, they develop standardized examination and diagnostic concepts and are active in research.
At the heart of the system is a digital input form that automatically takes gender-specific reference values into account. Before the examination, individual details such as gender, height, and weight are recorded. The system then displays the appropriate reference values for women or men and highlights abnormal findings in color. This allows changes to be detected more quickly and evaluated more precisely.
The underlying reference values are based on current recommendations from the German Society of Cardiology (DGK) and are continuously updated. The system is now used throughout the DHZC and supports uniform, gender-sensitive cardiac diagnostics.
Research shows that modern cardiology is becoming increasingly personalized. In addition to biological sex, other factors such as height, weight, and individual physical characteristics are increasingly being taken into account. The goal is more precise diagnosis and more personalized treatment of heart disease.
Cardiac Oncology: Where Cancer and Cardiology Meet
Cancer and cardiovascular diseases often influence one another. This is precisely what cardiac oncology focuses on—a specialized field at the intersection of oncology and cardiology. Researchers at the DHZC and at Charité are investigating how cancer treatments can strain the heart and how heart diseases affect the treatment of cancer patients.
A key focus of Dr. Ursula Wilkenshoff is on the question of how heart damage caused by modern cancer treatments can be detected early. This is because certain chemotherapies or radiation therapies can increase the risk of heart failure, arrhythmias, or vascular diseases.
Individual risk assessment is particularly important in this context. Women and men sometimes react differently to cancer therapies and may consequently develop different cardiovascular complications. The goal of the research is therefore to consider the heart and cancer therapy together and to provide patients with care as early as possible and on an individualized basis.
Cardioncology exemplifies how closely different medical specialties collaborate—and how important personalized medicine is for safe and long-term successful treatment.
Greater Diversity in Clinical Trials for Women's Cancer Research
Clinical trials are crucial for developing new cancer treatments. However, many studies have so far failed to adequately reflect the actual diversity of patients. People from different ethnic backgrounds, age groups, or socioeconomic backgrounds are often underrepresented. As a result, it is often unclear whether new treatments are equally effective and safe for all those affected.
An international team of researchers led by Prof. Jalid Sehouli (Director of the Charité Department of Gynecology at the Virchow Clinic Campus and first author of the publication) have therefore developed joint recommendations to make clinical trials in gynecological oncology more equitable and diverse. The goal is to remove barriers to participation in trials and to better translate research findings into real-world patient care.
The researchers emphasize that factors such as origin, ethnicity, age, or social living conditions can influence treatment outcomes. Nevertheless, these differences have not yet been adequately captured or evaluated in many studies. However, it is particularly important for personalized medicine to understand how different patient groups respond to therapies.
The recommendations of the international working group are intended to help make clinical research more inclusive and ensure that medical care is more equitable in the long term. At the same time, the work highlights the importance of diversity and gender-sensitive research in modern medicine—so that new therapies can benefit as many patients as possible.
Improving Diversity in Clinical Trials
Clinical trials form the foundation of modern medicine. To ensure that new therapies benefit as many people as possible, different population groups must be adequately represented in trials. However, this is often lacking: people from diverse social, cultural, or linguistic backgrounds have not participated equally in clinical trials to date.
International researchers from the network of theGynecologic Cancer Intergroup have therefore investigated the barriers that hinder participation in clinical trials and how diversity and equal opportunity can be improved. Prof. Jalid Sehouli, Director of the Charité Department of Gynecology at the Virchow-Klinikum Campus, is the last author of the publication.
Experts from 33 countries were surveyed for the study. The results show: Language barriers and strict inclusion criteria are among the most significant reasons worldwide for certain population groups being underrepresented in studies. A lack of information about clinical trials also makes it difficult for many people to access research.
It became particularly clear that women were more likely than men to support the proposed measures to improve diversity and participation. Providing study information in multiple languages was considered particularly helpful.
Research makes it clear that more equitable and diverse studies are necessary to better adapt medical care to different realities of life. The goal is research that takes all relevant population groups into account—thereby enabling more precise, fairer, and more personalized therapies.