Vascular loop
Unlike vascular rings, vascular loops do not completely surround the esophagus and trachea, but they can still compress them severely and cause symptoms.
Variants and causes
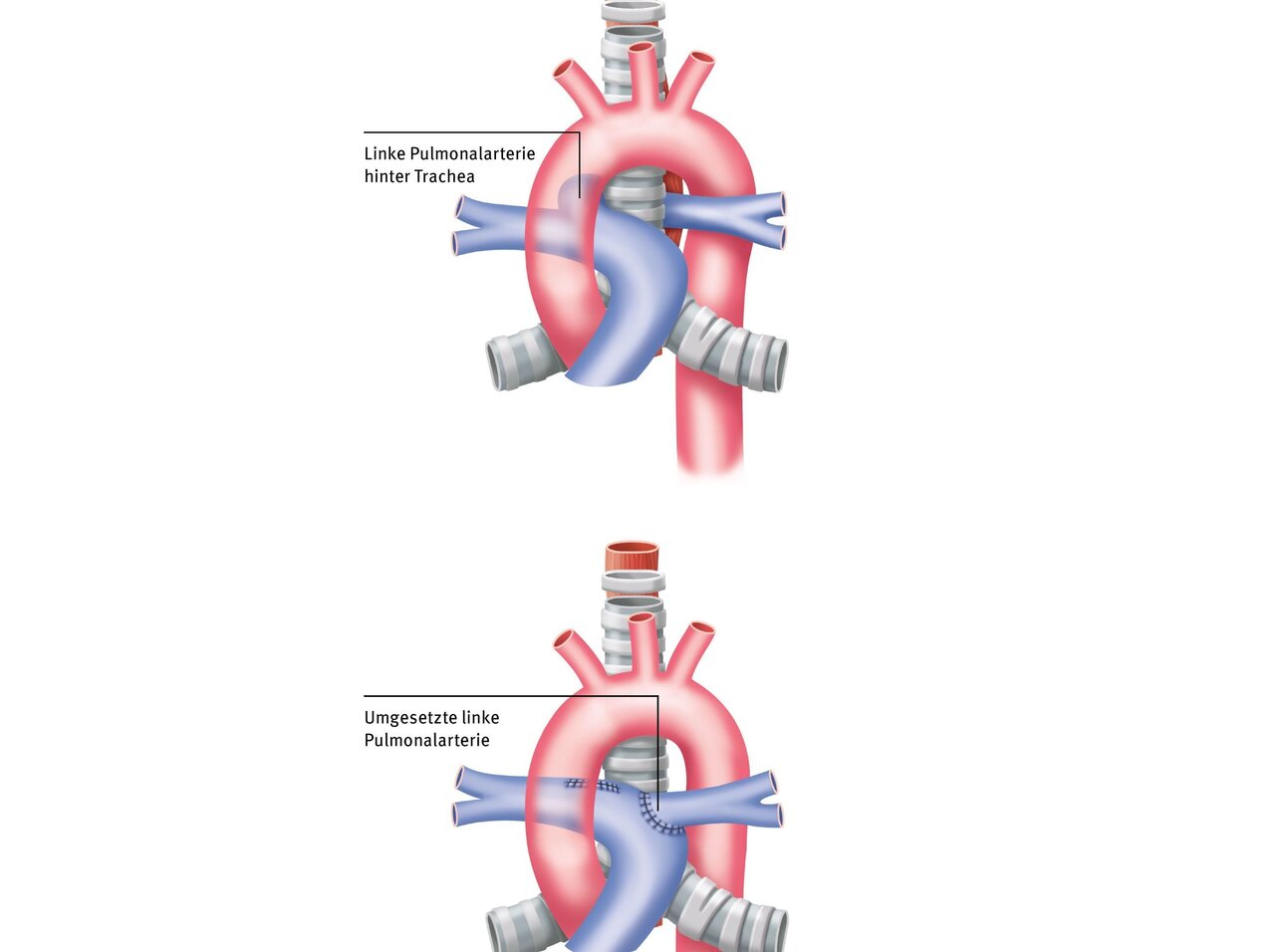
A typical example is the loop of the left pulmonary artery (LPA): The LPA first curves far to the right and then crosses between the esophagus and trachea to the left side. The abnormal path of the LPA between the esophagus and trachea causes constriction of the esophagus from the front and the trachea from the back. In addition, the LPA loop can occur in conjunction with a malformation of the trachea, in which the cartilage is formed as complete rings and may also be constricted.
Furthermore, the esophagus can be caused by a right subclavian artery (Arteria subclavia lusoria) that originates incorrectly from the descending aorta. In the area where the Arteria lusoria originates, the vessel can also be severely dilated (aneurysm), which can further exacerbate the symptoms. According to the first person to describe this condition, this enlargement or bulge is also known as Kommerell's diverticulum.
There is also the syndrome of compression of the brachiocephalic trunk, in which the trachea is constricted from the front by an artery (brachiocephalic trunk, which supplies blood to the right side of the head and neck and the right arm artery) due to a delayed departure of the trunk from the aortic arch.
A so-called loop of the aortic arch (circumflex aorta) is also very rare. In this case, there is a left aortic arch, but the descending aorta does not descend to the left, but crosses directly back to the right, which can lead to constriction of the windpipe or esophagus.
Symptoms
Normally, the trachea is held open in the front by cartilaginous rings. In the back, it is closed by a layer of muscle.
Due to the pressure of the vascular loop (typical in LPA sling and compression syndrome of the brachiocephalic trunk and in circumflex aorta) can cause narrowing and softening of the cartilage rings (tracheomalacia), which can lead to a typically exacerbated breathing sound (stridor) during inhalation and exhalation. Another reason for this breathing sound can also be a congenital narrowing of the windpipe (tracheal stenosis). In this case, the windpipe is often made up of complete cartilage rings instead of cartilage slats. Sometimes breathing difficulties are not recognized early on or are misinterpreted as asthma. In most cases of these vascular malformations, the body and lung blood flows do not mix, and therefore patients do not show signs of cyanosis or symptoms of heart failure such as sweating or poor growth.
The arteria subclavia lusoria causes difficulty swallowing because the artery (and possibly also the Kommerell diverticulum) crosses behind the esophagus, constricting it from behind.
Diagnossis
At the DHZC, we offer patients various diagnostic procedures. The diagnosis is often made during pregnancy using high-resolution ultrasound. After birth, the most important examination methods are: echocardiography, magnetic resonance imaging (MRI), computed tomography (CT) and bronchoscopy. This involves inserting a probe into the trachea to examine the narrowing and, if necessary, the entire cartilage rings. If the course of the vessels is unclear, angiography may also be necessary for clarification.
If the vascular loop is only detected after birth, magnetic resonance imaging (MRI) and computed tomography (CT) are particularly suitable for a clear diagnosis. These methods allow the organs and vessels to be reliably visualized.

If the vascular loop is only detected after birth, magnetic resonance imaging (MRI) and computed tomography (CT) are particularly suitable for a clear diagnosis. These methods allow the organs and vessels to be reliably visualized.
Therapy
After a median opening of the sternum, the malpositioned left pulmonary artery is detached from its connective tissue suspension. Once the heart-lung machine has been started, the left pulmonary artery can be separated from the right pulmonary artery and then pulled to the left side behind the trachea. The main trunk of the pulmonary artery is incised on the left and the left pulmonary artery is reattached to the correct (left) side of the main trunk. After cutting through the vascular loop, the reimplanted pulmonary artery may become constricted again during the course of the procedure.
If the narrowing is caused by softening of the cartilage rings of the trachea, the treatment consists of removing the constricting loop. Afterwards, there is often still a certain instability (softness) of the trachea, so that breathing difficulties may persist for some time even after the cause has been eliminated.
Sometimes, special reconstructive procedures on the trachea using a heart-lung machine are necessary to correct a long-distance narrowing.
In the case of the lusoria subclavian artery, a small incision (usually in the right armpit) is made to release the ductus band and the lusoria artery from the surrounding tissue and insert them into the right carotid artery. Any Kommerell's diverticulum is excised and sutured. The compression of the esophagus is relieved.
In brachiocephalic trunk compression syndrome, the artery supplying the right side of the head and neck and the right arm (brachiocephalic trunk) is detached using a heart-lung machine and then reimplanted further to the right in the aortic arch.
After a central opening of the sternum and start of the heart-lung machine, the left aortic arch and all vessels leading to the head are mobilized and then severed after the head and neck vessels have been disconnected. The aortic arch running behind the esophagus is pulled to the right side and reinserted on the right side of the ascending aorta. The narrowing is corrected.
Therapy at the DHZC
At the German Heart Center at Charité, we perform these very rare procedures on a routine basis. Even after corrective surgery, infants often require special intensive care follow-up, sometimes even a temporary tracheotomy. Our intensive care unit is staffed by pediatricians, pediatric intensive care physicians, and pediatric intensive care nurses with years of experience. They are familiar with these respiratory problems and can identify issues early on and treat them promptly.
Our extensive experience with such a rare and complex heart defect is reflected in the excellent postoperative progress of our patients. Further information can be found in our externally validated quality assurance standards and annual quality reports.
Forecast
The prognosis after correction of the vascular loop is generally good, and the symptoms are largely resolved. However, after the vascular loop has been severed, the reimplanted vessels may become narrowed again over time.
Therefore, in the weeks, months, and even years following the operation, regular check-ups with a pediatric cardiologist must be carried out in order to closely monitor further development and detect any narrowing.
When the sternum is cut lengthwise, it usually takes about four to six weeks to heal completely and become stable. After that, there is nothing to prevent normal physical activity.
Questions and answers for parents(FAQ)
If symptoms are present, corrective surgery should be performed promptly to avoid possible complications. The operation can be performed in early infancy without any increased risk.
Patients do not always experience symptoms in infancy. If symptoms are present, corrective surgery should be performed. A wait-and-see approach is not advisable, as the problem will not resolve itself.
