Aortic dissection
Cause, symptoms and surgery
Acute aortic dissection type A is one of the most urgent emergencies in cardiac surgery. Highly specialised experts with years of experience are available at the Deutsches Herzzentrum der Charité for every type of cardiac or vascular surgery, for intensive care, and for outpatient pre- and post-operative care.
Acute aortic diseases, including acute aortic syndrome, comprise various sudden conditions that often cause severe pain.
In aortic dissection, the innermost layer of the aortic wall tears, allowing blood to enter the space between the layers of the wall below.
(Image: Adobe Stock)
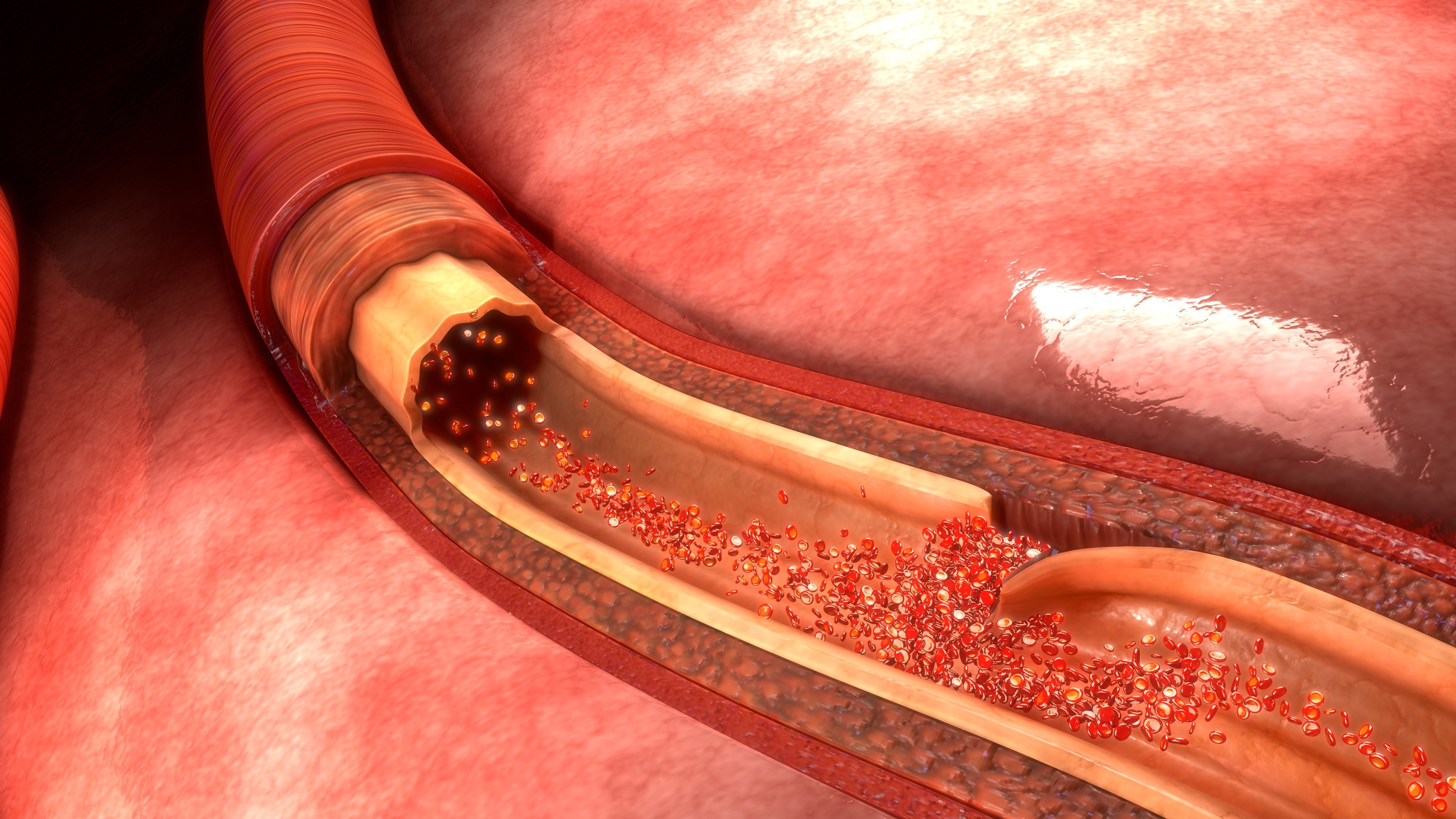
In aortic dissection, the innermost layer of the aortic wall tears, allowing blood to enter the space between the layers of the wall below.
(Image: Adobe Stock)
In classic aortic dissection, the innermost layer of the wall (intima) of the aorta tears, allowing blood to get between the underlying layers of the wall and ‘burrow’ there. This causes the wall layers to separate; a new, blood-filled vascular space (so-called false lumen) develops next to the actual vascular interior (so-called true lumen). Vessels that branch off from the aorta, e.g. to the head or the coronary arteries, can be compressed as a result or no longer receive enough blood to supply the respective organs.
Depending on the affected vessel, this reduced blood flow causes various symptoms. Most patients report sudden onset of severe pain with a ripping or stabbing character. If the dissection progresses along the aorta, the pain (nailing pain) is also perceived as migrating.
Aortic dissection is classified according to its location. The most common classification is the so-called Stanford classification. This differentiates between type A and type B dissections.
Type A aortic dissection
In type A dissection, bleeding begins in the ascending aorta and can spread over the entire length of the aorta. Acute type A dissection is a life-threatening emergency and requires immediate surgical treatment at a cardiac surgery centre. The mortality rate in the first 48 hours is very high (1-2% per hour). Depending on the location of the dissection, the consequences can include heart attacks, strokes, paralysis or insufficient blood supply to internal organs.
If the outermost aortic wall layer can no longer withstand the pressure of the ‘trench bleeding’ and also tears, an aortic rupture occurs. This usually leads to immediate death. Hemorrhage into the pericardium is also a dreaded complication, as this constricts the heart and thus it can no longer beat effectively (so-called cardiac tamponade).
Type B aortic dissection
A type B dissection is when the dissection starts after the left subclavian artery (arteria subclavia sinistra) in the descending part of the aorta (aorta descendens).
Type B dissection is less common than type A dissection. The risk of sudden rupture is lower because blood pressure is lower in the descending part of the aorta. Chronic aortic dissection Like aortic aneurysm, chronic aortic dissection is a slowly progressive disease of the aorta. It is very important to have regular check-ups and to see a doctor immediately if any new acute symptoms occur.
Chronic aortic dissection
Like aortic aneurysm, chronic aortic dissection is a slowly progressive disease of the aorta. It is very important to have regular check-ups and to see a doctor immediately if any new acute symptoms occur.
In the case of an aortic dissection, the innermost layer of the wall (intima) of the aorta tears, allowing blood to enter the space between the layers of the wall below it. This causes the layers of the wall to separate, creating a new, blood-filled vessel space (so-called false lumen) next to the actual vessel interior (so-called true lumen). As a result, vessels branching off from the aorta no longer receive sufficient blood to supply the organ.
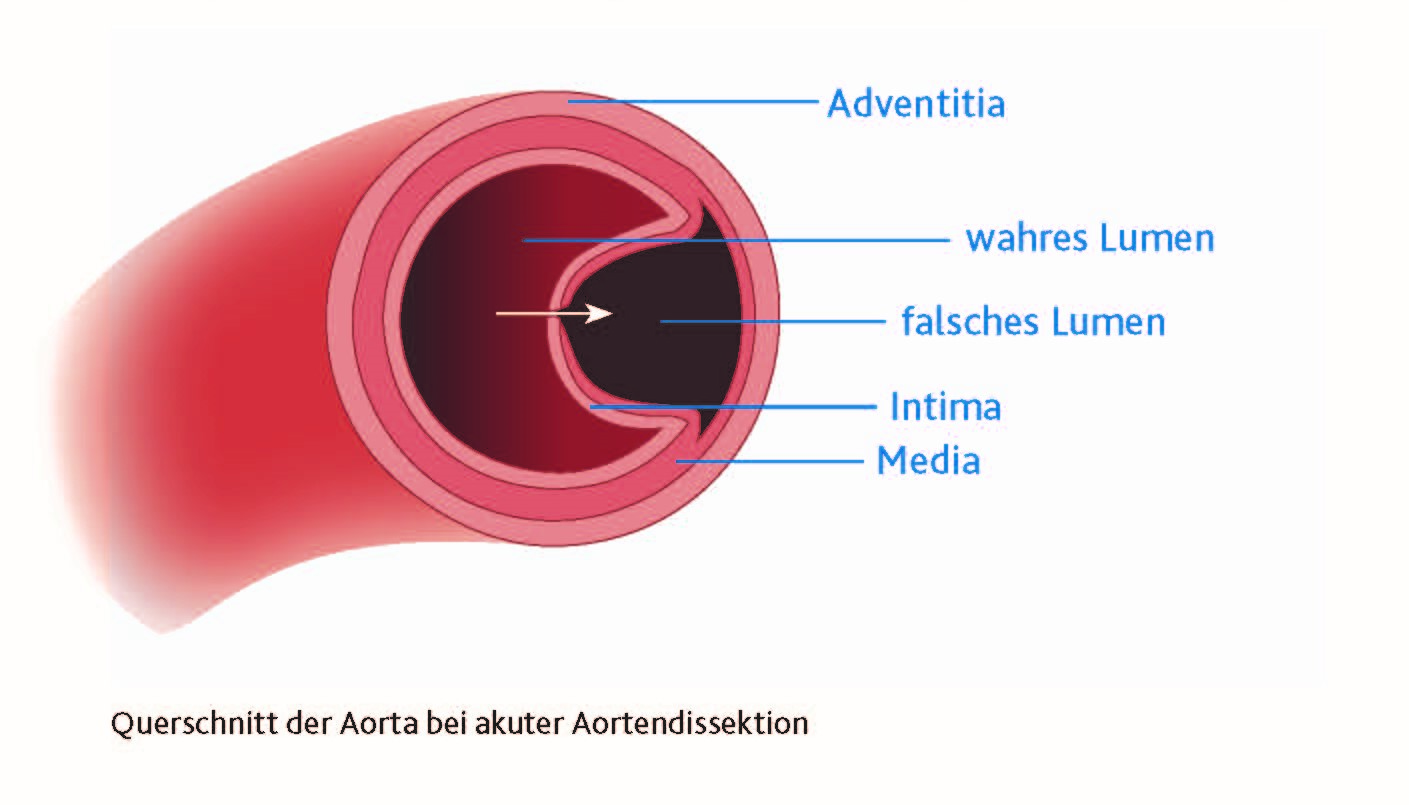
In the case of an aortic dissection, the innermost layer of the wall (intima) of the aorta tears, allowing blood to enter the space between the layers of the wall below it. This causes the layers of the wall to separate, creating a new, blood-filled vessel space (so-called false lumen) next to the actual vessel interior (so-called true lumen). As a result, vessels branching off from the aorta no longer receive sufficient blood to supply the organ.
Why some people experience a weakening of the inner walls of the aorta, which can even lead to tears, is not yet fully understood. Current studies show a frequency of up to 12 cases per 100,000 inhabitants. Men are affected up to three times as often as women. The average age of those affected is around 60 years. For unknown reasons, aortic dissections tend to occur more frequently during the winter months. It is also unclear why most dissections occur in the morning between 6:00 a.m. and 12:00 p.m.
A number of factors increase the risk of aortic dissection, for example, untreated or inadequately treated high blood pressure, smoking, and various connective tissue diseases such as Marfan syndrome or Ehlers-Danlos syndrome.
A team from the Department of Cardiothoracic and Vascular Surgery at the DHZC (Director: Prof. Dr. Volkmar Falk), led by Stephan Kurz, analysed the patient files and emergency physician protocols of over 1,600 patients treated at the DHZC for acute type A dissection.
In addition, more than 14,000 autopsy reports were examined to determine how many patients in Berlin and Brandenburg died from aortic dissection who could not be operated on in time. The results were published in the renowned ‘International Journal of Cardiology’ and show an urgent need for action. The study found
- that the median time from the onset of symptoms to the start of surgery is over 8 hours.
- that aortic dissection is much more common than previously thought: the German Federal Statistical Office assumes 4.6 cases per 100,000 inhabitants annually; the extrapolation of the data collected in the study results in a value that is more than twice as high (11.9 cases).
Symptoms and diagnosis
A sudden, crushing pain, usually in the chest but often radiating to the back and abdomen, is typical of an aortic dissection.
If you experience these symptoms, always contact an emergency doctor immediately and describe them.
Depending on which of the blood vessels branching off from the aorta are closed off by the dissection, symptoms of reduced blood supply to the affected organs may also occur. This manifests itself in the form of severe abdominal pain in the event of circulatory disorders in the intestines or kidneys. In some cases, circulatory disorders can also lead to symptoms of a stroke.
The clinical picture of an aortic dissection is tricky because it can easily be misinterpreted by emergency physicians as a heart attack (which occurs much more frequently), which in the worst case can lead to incorrect initial treatment. However, known risk factors, such as pre-existing conditions or previous aortic surgery, but also special findings during the initial examination, such as a difference in blood pressure between both arms, in combination with the typical pain pattern, indicate an acute aortic dissection.
Any sudden severe pain in the back, chest or abdominal area for which no other plausible explanation can be found should therefore also lead to aortic dissection or an aortic aneurysm being considered.
A reliable diagnosis is usually only possible with the help of computed tomography.
Therapie
The only possible treatment for acute aortic dissection is immediate open-heart surgery. Specialised teams can perform these operations at DHZC at any time in state-of-the-art operating theatres.
(Image: DHZC/Külker)

The only possible treatment for acute aortic dissection is immediate open-heart surgery. Specialised teams can perform these operations at DHZC at any time in state-of-the-art operating theatres.
(Image: DHZC/Külker)
Type A aortic dissection
With every hour that acute type A aortic dissection remains untreated, statistically two percent of patients die.
The only possible treatment for acute aortic dissection is immediate open-heart surgery, which must be performed by a trained and well-coordinated team of surgeons, perfusionists, anaesthetists and surgical nurses.
The heart surgeon opens the patient's chest, after which the patient is connected to a heart-lung machine and the heart is shut down. The subsequent surgical treatment depends on the location and extent of the aortic dissection. In most cases, the affected section is replaced by a vascular prosthesis, and an artificial aortic valve may also need to be inserted. After the operation, the patient continues to receive intensive medical care.
The Deutsches Herzzentrum der Charité is one of the few clinics that can treat acute aortic dissection surgically at any time, as specialised teams are available around the clock. With well over a hundred operations a year, the DHZC is one of the largest centres in Germany for this type of surgery.
We have compiled detailed information for you on the various surgical methods, the requirements for surgery and life after surgery on the page aortic surgery.
We have summarised the various surgical methods, the requirements for an operation and life afterwards for you in detail on the aortic surgery page.

Type B aortic dissection
Type B dissection can be divided into two groups: an "uncomplicated" and a "complicated" form.
In an "uncomplicated" type B dissection, no surgical intervention is usually necessary. Instead, the blood pressure, heart rate and pain are treated with medication. The progression of type B dissection should also be counteracted by minimising the risk factors. Regular check-ups by the doctor (including imaging) are important in order to be able to intervene quickly in the event of relevant changes to the aorta.
In "complicated" type B dissection, the pain often persists. Blood pressure is also difficult to adjust. This is associated with a rapid expansion or even rupture (tear) of the aorta. In addition to lowering blood pressure, minimally invasive treatment using stent implantation (TEVAR) is recommended in this case. If this treatment is not possible, open surgery is performed.
Stents in the thoracic aorta (thoracic aorta) are called TEVAR (thoracic endovascular aortic repair), in the abdominal aorta (abdominal aorta) EVAR (endovascular aortic repair).
Genetic examination
Aortic aneurysms and dissections can occur in conjunction with genetic, congenital connective tissue diseases or syndromes. However, their severity can vary greatly. When a human genetic examination makes sense must always be decided on an individual basis. These tests are recommended for relatively young patients with aortic disease, as this can have consequences for their aftercare and also for close relatives.
The Marfan Centre at the German Heart Centre of the Charité (DHZC) emerged from the special Marfan consultations that have existed for over twenty years in the Human Genetics Department at the Charité and the Cardiac Surgery Department at the DHZC. A legal regulation (§ 116b SGB V) for the outpatient care of patients with rare diseases such as Marfan syndrome makes it possible to offer complex care and treatment under one roof. This is where the experience of the doctors comes together.
Ideally, patients can attend all necessary appointments at the Marfan Centre in a short space of time.
Outpatient clinic and consultation hours
Aortic consultation hours of the cardiac surgery outpatient clinic at the German Heart Centre of the Charité:
Tel +49 30 4593-2002
Marfan Centre of the Charité and the German Heart Centre of the Charité - Outpatient consultation for patients with genetic aortic diseases:
Tel +49 30 450 665 356
Email: marfan@charite.de
The authors

Dr. med. Semih Buz works as a senior physician at the Department of Cardiac, Thoracic and Vascular Surgery at the German Heart Centre of the Charité (DHZC). He is head of the vascular surgery department.
